Pros and Cons of Omega Q Plus Resveratrol Reviews
Today, Americans often accept vitamins, herbs and other sup-plements—and they're unremarkably aware of many more than that they may not actu-marry exist taking. So it's no surprise that our patients sometimes ask our opin-ion on the value of these supplements, in detail how they may or may not impact glaucoma. Furthermore, with marijuana becoming legal in more and more than states, questions nearly its reputed ability to lower intraocular pressure level are likely to come too.
Our patients look to us for show-based data most these substances. Hither, I'd similar to review a little bit of what the studies to engagement have shown, to offer some guidance regarding what you lot might want to say to your patients when these questions arise.
The Value of Vitamins
It'due south non unreasonable to believe that supplements such as vitamins could bear upon the progression of glaucoma. Doctors dealing with age-related macular degeneration have already demonstrated the potential of this approach. As we all know, the Age- Related Middle Disease Study found that a combination of antioxidants and zinc was able to reduce the progression of disease in macular degeneration patients with intermediate and big drusen past 25 percent,ane so it is possible to find something in the world of complementary and alternative medi-cine that can help address heart disease. In glaucoma, we simply haven't notwithstanding found the perfect mixture. The reason for that may be, in role, that glaucoma is actually a cluster of related diseases. Treating it may ultimately involve addressing both pressure bug and neuroprotective issues.
Vitamin supplements that have been posited to take an event on glaucoma include B1, B3, B12, C, A and E. The chart on the facing folio shows some of the studies, pro and con, apropos five of the most commonly taken vitamins. Notably, the results of different studies are often contradictory.
A few observations:
• Vitamin B1 (thiamine) . Edward Asregadoo, MD, theorized that B1-deficient patients might be more prone to glaucoma. He noted that low levels of vitamin B1 are associated with increased cortisol, which in turn increases IOP. A study he published did find lower serum thiamine in glaucoma patients.ii However, vitamin B1 didn't significantly lower IOP, and unfortunately, the study wasn't well-designed. Other show suggests that B1 levels may not bear upon glau-coma; alcoholics, for example, tend to be deficient in vitamin B1, but there's no correlation betwixt alcoholism and glaucoma.
• Vitamin C . The show for vitamin C's impact on glaucoma is mixed. Ane study found that intra-venous vitamin C lowered IOP xx percent over two hours; it does announced to have a meaning osmotic effect, similar to mannitol.3 Still, IOP climbs back up over 10 to 12 hours, and it's not really practical to give someone 4 vitamin injections. Other studies, looking at vitamin C supplements, didn't evidence much of a alter in force per unit area.4,5 And while vitamin C has a beneficial reputation, it can crusade kidney stones and gastrointestinal upset, and information technology should be avoided in those with a glucose-6-phosphate dehydrogenase (G6PD) deficiency, B-thalassemia or hemochromatosis.
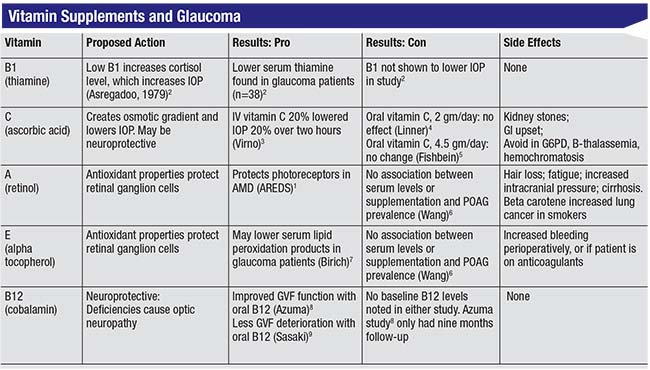
• Vitamin A (retinol) . Every bit an anti-oxidant, vitamin A might be expected to protect retinal ganglion cells, and the AREDS written report did find evidence that it protects photoreceptors in macular degeneration patients. However, a study by Sophia Wang, MD, establish no association between vitamin A supplementation or serum levels and principal open-angle glau-coma prevalence.half-dozen Meanwhile, retinol can have side effects including hair loss, fatigue, increased intracranial pressure and cirrhosis.
• Vitamin E (alpha tocopheral) . Vitamin Due east does accept antioxidant properties, and one study plant that it may lower peroxidation products in glaucoma patients.seven However, the previously mentioned report by Dr. Wang6 found no association between vitamin Due east and glaucoma prevalence, and vitamin E tin potentially cause increased haemorrhage perioperatively, besides as in patients already taking an anticoagulant.
• Vitamin B12 (cobalamin) . B12 is neuroprotective, and we know that deficiencies in B12 are associated with optic neuropathy. Two studies found visual field improvement with vitamin B12 supplementation,eight,9 but no baseline B12 levels were done in these studies, and they had very short follow-upward.
Other supplements have produced interesting results in animals and in in vitro studies. Vitamin B3 (nicotina-mide), for example, may be neuro-protective. One animal written report reported in Science10 found that vitamin B3 could help to mitigate mitochondrial dysfunction, which has been linked to retinal ganglion prison cell damage and death. In this written report, mice were fed a supplement equivalent to 2.5 grams a day in humans; information technology prevented the structural and functional loss of ganglion cells and nerve axons, and the effect persisted, even with elevated pressure. Furthermore, intravitreal injections of a gene that produces nicotinamide protected lxx percentage of mice from glaucomatous damage for 12 months. In improver, combining the two approaches provided more protection than either one alone. So in vitamin B3 nosotros take the potential for an agent that not simply has a neuroprotective consequence but tin can besides continue having that protective effect in the presence of elevated pressure. The idea that nicotinamide may have benign effects has been proposed for farther investigation in humans.eleven And then far, nonetheless, this has merely been shown in animal studies.
One of the main bug with vitamin studies is that studies tend to involve very small numbers of patients, and a lot of the reports accept been anecdotal. The reality is that since the U.S. Food and Drug Admin-istration doesn't need to approve any of these agents, there'south no incentive for large studies to exist conducted, the way there might be with drugs that need FDA approval. Every bit a result, very few large, controlled studies take been done.
In that location'southward also another meaning trouble: Many of these studies are washed in vitro, where, for instance, the amanuensis may protect ganglion cells.
Simply when a person ingests a supplement, information technology has to go through all of the metabolic processes in the body, so the potency could be significantly diminished by the time it gets to the nerve cells. That makes it difficult to know what the proper dose should be for humans.
Other Supplements & Nutrients
The trouble of potency following ingestion is an issue with two non-vitamin supplements that have shown hope with glaucoma: co-enzyme Q and resveratrol. These have been shown to reduce mito-chondrial susceptibility in vitro, and I believe they show promise for neuro-protection.
One study found that topical micelles of co-enzyme Q10 with vita-min E d-a-tocopheryl polyethylene glycol 1000 succinate, twice a 24-hour interval, significantly reduced the number of apoptotic retinal ganglion cells three weeks after induction of ocular hypertension. Furthermore, the issue was independent of IOP.12 Another report institute that resveratrol retarded apoptosis of RGS'south in vitro and decreased the level of caspace-iii (a marker of apoptotic events), while stimulating increased quantities of mitochondria.13 Unfortunately, when a person ingests co-enzyme Q or resveratrol in supplement form, the efficacy may be dramatically altered by the metabolizing procedure. Clinical trials in humans could practice a lot to pin downward the quantities and con-centrations required to produce simi-lar effects in our patients.
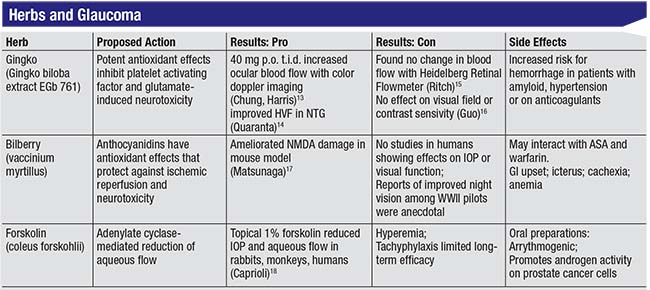
A few herbal supplements are as well believed to have positive furnishings on the eyes and glaucoma. The chart above shows some of the data relating to three popular herbal supplements that sources on the Internet claim volition help treat glaucoma.
A few observations almost these three herbal supplements:
• Gingko biloba . This is a well-known antioxidant used widely in Europe to treat animate issues and Reynaud'south phenomenon, which is a vascular disorder. Gingko is known to inhibit glutamate cytotoxicity, which leads to ganglion cell death, and it's been shown to increase blood flow.14,fifteen Yet, these were very small studies, and there were a couple of contrasting studies that found no event on visual field or dissimilarity sensitivity, as well as one that institute no change in blood flow.16,17 One of the challenges when studying gingko's effect on claret menses is that we still don't have understanding on the best way to mensurate ocular blood menses, making it difficult to draw whatsoever conclusions nigh how helpful gingko actually may exist.
Ane other important consideration when suggesting that a patient try gingko: Gingko increases the take a chance of bleeding. For that reason, you take to brand certain your patient is not on warfarin, aspirin or any other blood thinners, because your patient could be prone to getting pretty severe hemorrhages.
• Bilberry (vaccinium myrtillus). The bilberry plant is a cousin of the blueberry. In World War Two, fighter pilots took bilberry to increment their dark vision, only to date, no study has been done to confirm that this effect is existent. As an anthocyanidin, bilberry has a very potent antioxidant effect that tin can protect against ischemic reperfusion and neurotoxicity, and it's been shown to subtract retinal ganglion cell impairment in a mouse model.18 However, no studies in hu-mans have shown any effect on IOP or visual office. Bilberry tin can also interact with aspirin and warfarin and potentiate bleeding; and it has been associated with gastrointestinal upset, icterus, cachexia and anemia.
• Forskolin (coleus forskohlii). This herb has been shown to lower IOP in rabbits, monkeys and humans by reducing aqueous menses. This was first demonstrated back in the mid-1980s.19,20 However, further studies were abandoned because forskolin caused significant hyperemia and tachyphylaxis. Furthermore, after a calendar month or two the force per unit area would shoot back up, so in that location wasn't a lot of long-term promise. Oral preparations are available, just when you take forskolin orally information technology doesn't have whatsoever effect on IOP. Downsides include that forskolin is arrythmogenic, and information technology tin can promote androgen activity on prostate cells in patients with prostate cancer.
Some food-rich foods show promise for impacting glaucoma progression. The Osteoporotic Fractures Inquiry Group establish that patients who ate iii or more servings of fruit such as peaches or oranges, or fruit juices, per day were 79 percent less likely to take POAG. In add-on, those who ate more than one serving of collard greens or kale, which are nitrate-rich, leafy green vegetables, per calendar week decreased their odds of having POAG by 57 per centum.21,22 The Nurses Health Report and Health Pro-fessionals Follow-up Study found that a greater intake of nitrate-rich foods and leafy green vegetables decreased the risk of POAG by 20 to 30 percent.23 These are large, well-designed population studies. Gran-ted, they were large cohort studies that relied on statistical analysis, and the data was based upon patient self-reporting, so they could contain an element of bias. It'due south besides possible that individuals eating large quantities of these foods may have a healthier lifestyle overall, and that might be contributing to their reduced POAG. However, the statistics are pretty impressive.
Ane of the take-domicile messages here is that although we often hope to go relief from supplements in pill form, there may be an advantage to ingesting beneficial nutrients in their natural dietary form. Other pro-nutrients in these vegetables and fruits may also be contributing protective furnishings.
Medical Marijuana
The herb patients most often enquire about, not surprisingly, is marijuana. Medical marijuana is currently legal in 30 states, including the District of Columbia, and recreational marijuana is legal in a scattering of states, about recently California (every bit of January 1, 2018). The interesting matter about marijuana is that it's a Schedule I con-trolled substance, while
 |
| Although early studies suggested that marijuana may reduce IOP for a few hours, a host of side effects and applied concerns make its utilize as a glaucoma treatment controversial at best. |
opioids, amphetamines and cocaine are Schedule Ii. That means that, unlike marijuana, they're available for inquiry.
The original studies on marijuana were done dorsum in the 1970s.24 Those studies, using a small sample of participants, showed a significant reduction in IOP (25 to thirty percent) in 65 per centum of patients. However, participants' eyes got red, tear product decreased, pupils got smaller, and the decrease in pressure level simply lasted 3 to four hours. It's too difficult to evaluate these studies relative to today's marijuana use considering marijuana authorization is difficult to verify. In the early studies, individuals were smoking 2% marijuana cigarettes; today the concentration of THC in a marijuana cigarette may be much higher.
A few years later, Keith Green, PhD, did similar studies using oral ingestion (e.g., eating marijuana brownies).25 The results were mixed; in some patients this lowered IOP, but in others information technology didn't. In any case, oral ingestion requires larger quantities of the drug to produce the aforementioned event, which makes sense because the drug is being taken in through the alimentary canal where it must be metabolized past the liver, etc. That's going to decrease the potency and availability of any active compounds.
Of course, marijuana can have numerous side effects. These include ocular side furnishings such as conjunctival hyperemia, decreased lacrimation, diplopia, impaired accommodation, photophobia, nystagmus and bleph-arospasm. Systemic side furnishings in the curt term may include increased pulse, orthostatic hypotension, and of course, euphoria.26 Over the long term, side furnishings may include emphy-sema-like lung changes, decreased immune function, decreased cognitive function and potential alterations in the growth of a fetus. (Information technology would be helpful to comport long-term studies, but as long every bit marijuana remains a Schedule I agent, that'south unlikely to happen.)
Encouraging patients to fume marijuana to address glaucoma is controversial at all-time. Smoking inher-ently carries some gamble for emphysema and lung cancer, along with the other same side effects. The orthostatic hypotension event may also be significant, because of the likelihood that the drug is decreasing blood menses to the optic nerve, which could exist damaging. The CNS side effects are problematic, peculiarly for older patients. Moreover, current topical medications usually accept a better efficacy profile for lowering IOP. For all of these reasons, both the American Academy of Ophthalmology and the American Glaucoma Society currently do not recommend the employ of marijuana to treat glaucoma.
A promising approach in the future may exist the use of cannabinoids, the agile compounds institute in mari-juana, which are receiving research attention. Cannabinoids such as delta9-THC and cannabidiol accept been shown to decrease IOP; they act on cannabinoid receptors in the trabecular meshwork and increment aqueous outflow, and they also have neuroprotective qualities. Ane study of WIN55212-ii found that it decreased IOP 20 to thirty percent, achieving maximum effect within 60 minutes, although the issue did not last long.27
Some more than recent research involving THC prodrugs such every bit THC-Val-HS has been more promising. Coupling the drug with cyclodextrins and surfactants helps to increase solubility, so there's more availability and better penetration through the cornea. In a rabbit model this produced a better IOP lowering than timolol, although information technology had a shorter duration of activeness, similar to pilocarpine.28
The main betoken is, while smoking marijuana isn't something that we equally ophthalmologists currently stand behind, cannabinoid agents may have the potential for ocular penetration without the potential for side effects such as orthostatic hypotension and euphoria. In the meantime, the potential for benefits from the occasional adjunctive employ of marijuana in add-on to prescribed glaucoma treatment regimens, and the effects of marijuana in glaucoma patients who regularly apply it for nonmedical reasons, have not been investigated.
Managing Patient Questions
Patients enquire me about smoking marijuana all the time; they want me to prescribe it for them. If yous haven't already encountered this, you probably will.
Here are a few strategies that may assist you manage this situation when it arises:
• Be aware of the marijuana laws in your state. Apply of marijuana, even for medical reasons, is subject to law. To keep yourself and your patients out of trouble, do your homework well-nigh the legal ramifications in your state.
• Exist ready with an answer be-fore your patients ask questions. I explain to my patients that so far information technology'south non clearly divers how marijuana should be used to treat glaucoma. Even though it'south approved for glaucoma treatment here in Florida, there are no guidelines. In addition, the American Academy of Ophthalmology and American Glaucoma Lodge exercise not advocate its use for treating glaucoma. For these reasons—amid others—the majority of doctors I know won't prescribe information technology. (I don't, either.)
• Brainwash and inform interested patients regarding the efficacy, side effects and drug interactions associated with marijuana use. Most interested patients take trivial, if any, idea about this aspect of marijuana use. It'due south worth pointing out that while marijuana may lower IOP in the short term, in the long term it may do them more impairment than good.
• Consider prescribing an oral cannabinoid like Marinol (dronabinol) instead. Marinol has been used for decades in cancer patients to care for nausea and other gastrointestinal side furnishings of chemotherapy. The few times I've prescribed it for patients, it's had a modest result on IOP, lowering information technology x to xv percentage. Notably, it appears that it'south non completely costless of the euphoric effects. Some patients complain that they still experience effects such as lightheadedness or confusion—while other patients are not bothered at all. (Hopefully the research into topical cannabinoids will bear fruit, thus taking any systemic side effects off the tabular array.)
Playing It Condom
Given the popularity of supplements and marijuana today, it'due south essential that nosotros exist prepared to help our patients navigate the rational use of these substances. We have to exist set to brainwash patients on their efficacy and side furnishings. A few points worth making:
• Patients should be careful with any of these supplements considering even if they may potentially help, no ane knows the proper dosage. The reality is, these treatment possibilities haven't been seriously studied, so nosotros're making choices based on minimal information.
• Exist careful virtually the purity of the substance in question. Many herbs are sold mixed with other herbs, and some individuals can have pretty dramatic side furnishings from those additional herbs.
• Do your homework earlier proceeding. Your patients should talk to their internist if they're planning on using supplements, to brand sure they don't interact with any prescription drugs they may be taking. Some supplements volition collaborate with blood thinners, or may exacerbate other problems like prostate cancer or gastrointestinal issues. While some supplements may be helpful, they are not totally beneficial.
• Encourage a healthy diet with antioxidant and nitrate-rich foods including citrus fruits, peaches, salad, kale and collard greens. These foods not only limit the possibility of side effects, they have some of the well-nigh impressive supporting evidence in the literature. Citing some of the statistics establish in the research may surprise and impress your patients. REVIEW
Dr. Gamell is an associate professor of ophthalmology at the Academy of South Florida Health Morsani College of Medicine, and Glaucoma Fellowship Director at the USF Center Institute in Tampa.
i. Historic period Related Eye Illness Study Grouping. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and Due east, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch Ophthalmol 2001;119:ten:1417-1436.
2. Asregadoo ER. Blood levels of thiamine and ascorbic acrid in chronic open-angle glaucoma. Ann Ophthalmol 1979;xi:1095–1100.
3. Virno Thousand, Bucci MG, et al. Intravenous glycerol-vitamin C (sodium common salt) equally osmotic agents to reduce intraocular force per unit area. Am J Ophthalmol 1966;62:824–833.
4. Linner E. The force per unit area lowering effect of ascorbic acid in ocular hypertension. Acta Ophthalmol (Copenh) 1969;47:685–689.
v. Fishbein SL, Goodstein South. The pressure lowering effect of ascorbic acid. Ann Ophthalmol 1972;4:487–491.
6. Wang SY, et al. Glaucoma Vitamins A, C, and E supplement intake and serum levels in a population-based sample of the United States. Eye 2013; 27:4:487-494.
7. Birich TV, Birich TA, Marchenko LN: [Vitamin E in multiple-modality treatment of primary glaucoma patients]. Vestn Oftalmol 1984;102:ten–3.
8. Azumi I, Kosaki H, Nakatani H. Effects of metcobolamin (Methycobal) on the visual field of chronic glaucoma—a multicenter open study. Folia Ophthalmol Jpn 1983;34:873–878.
ix. Sasaki T, Murata Thou, Amemiya T. Effect of long-term handling of glaucoma with vitamin B-12. Glaucoma 1992;fourteen:167–170.
10. Williams PA, et al. Vitamin B3 modulates mitochondrial vulnerability and prevents glaucoma in aged mice. Science 2017;355:756-760.
xi. Williams PA, Harder JM, John SW. Glaucoma as a metabolic optic neuropathy: Making the instance for nicotinamide treatment in glaucoma. J Glaucoma 2017;26;12;1161-68.
12. Davis BM, et al. Topical Coenzyme Q10 demonstrates mitochondrial-mediated neuroprotection in a rodent model of ocular hypertension. Mitochondrion 2017; 36: 114-123.
13. LiuXQ, Chen MM, et al. Resveratrol Mitigates Rat Retinal Ischemic Injury: The roles of matrix metalloproteinase-9, inducible nitric oxide, and heme oxygenase-1. Jour Oc Pharm Ther 2013;29:1:33-40.
xiv. Chung HS, Harris A, et al. Ginkgo biloba extract increases ocular blood period velocity. J Ocul Pharmacol Ther 1999;15:iii:233-twoscore.
15. Quaranta LR, et al. Ginkgo biloba extract improves visual field harm in some patients affected by normal-tension glaucoma. Invest Ophth Vis Sci 2014;55:2417.
xvi. Gurses-Ozden R, Harris A, et al. Ginkgo biloba extract does not alter peripapillary retinal hemodynamics using Heidelberg Retina Flowmetry in open-angle glaucoma. Invest Ophthalmol Vis Sci 2002:42(Suppl)
17. Guo X, et al. Author Response: Event of Ginkgo biloba on visual field and contrast sensitivity with NTG in Chinese patients: A randomized, crossover clinical trial. Invest Ophth Vis Sci 2014;55:110-116.
18. Matsunaga North, et al. Bilberry and its master constituents take neuroprotective effects against retinal neuronal harm in vitro and in vivo. Mol Nut Food Res 2009;53:vii:869-77.
19. Caprioli J and Sears M. Forskolin lowers intraocular pressure in rabbits, monkeys, and man. Lancet 1983;one:958-960.
20. Caprioli J, et al. Forskolin lowers Intraocular force per unit area past reducing aqueous arrival. Inves Ophthalmol Vis Sci 1984;25:268-277.
21. Coleman AL, Rock KL, Kodjebacheva G, et al. Glaucoma hazard and the consumption of fruits and vegetables amid older women in the study of osteoporotic fractures. Am J Ophthalmol 2008;145:half-dozen:1081–1089.
22. Giaconi JA, et al. The association of consumption of fruits/vegetables with decreased risk of glaucoma among older African–American women in the report of osteoporotic fractures. Amer J Ophthal 2012;154:iv:635-644.
23. Kang, JH, et al. Association of dietary nitrate intake with primary open-angle glaucoma, a prospective analysis from the Nurses' Health Study and Health Professionals Follow-upward Report. JAMA Ophthalmology 2016;13:3:294-303.
24. Hepler RS, Frank IR. Marihuana smoking and intraocular pressure. JAMA 1971;217:1392.
25. Green K. Marjuana smoking vs cannabinoids for glaucoma therapy. Arch Ophthalmol 1998;116:1433-1437.
26. Merritt JC, et al. Effect of marijuana on intraocular and blood pressure in glaucoma. Ophthalmology 1980;87:3:222-viii.
27. Porcella A, Maxia C, Gessa GL, Pani Fifty. The synthetic cannabinoid WIN55212-2 decreases the intraocular force per unit area in human glaucoma resistant to conventional therapies. Eur J Neurosci 2001;thirteen:ii:409-12.
28. Adelli GR, et. al. Development of a delta9-tetrahydrocannabinol amino acrid-dicarboxylate prodrug with improved ocular bioavailability. Inves Ophth Vis Sci 2017;58:4:2167-2179.
hewettswitted1985.blogspot.com
Source: https://www.reviewofophthalmology.com/article/supplements-and-glaucoma-advising-your-patients
0 Response to "Pros and Cons of Omega Q Plus Resveratrol Reviews"
Postar um comentário